MANAGEMENT OF BRAIN DEATH

MISCELLANEOUS PROBLEMS Infection Systemic infection is a relative contraindication to organdonation. All unnecessary indwelling devices should be removed. All lines and catheters must be inserted aseptically and meticulous care of dressings and wounds is vital. Tracheal suction should be done withsterile precautions. Appropriate samples from suspected sources of infection should be sent for cultures. Treatment should be initiated based on culture reports. Prophylactic antibiotics are indicated only immediately prior to organ retrieval.
Coagulopathy Disseminated intravascular coagulation is common in patients with traumatic head injuries. This is due to the release of thromboplastin from the injured brain. If it results in clinically significant mucocutaneous bleeding, treatment with appropriate blood components is needed.
Hypothermia Core temperature should be monitored using rectal thermometers. The core temperature should be maintained above 350C after brain death, the body becomes poikilothermic because of the loss of central temperature control mechanisms. Treatment includes use of humidified and warmed ventilator gases ; warmed intravenous fluids and blood products ; and heating blankets. Sometimes a hot blower next to the patient is the best solution to maintain the body temperature.
Brain stem dead organ donors are managed in the intensive care unit. Supportive care is directed towards optimizing organ function as this will improve graft survival and function.
CONCLUSION: A severe shortage of organs the world over has led to increased pressure on the intensive
care staff for early identification of the brain dead donor and optimum management of
this condition. The diagnosis of brain death as per the Transplantation Human Organ Act
is based as simple clinical bedside tests. The passing of this Act in 1994 and its
subsequent adaptation by many Indian States has made it possible in India to use this
pool of patients for organ retrieval and transplantation.
Table 1. States that have accepted THO Act Table II. Form VIII of Transplantation of Human Organ Act
| S.No |
Brainstem Reflexes |
Sensory cranial nerve |
Motor cranial nerve |
| 1. |
Absence of pupillary response to light |
II |
III (parasympathetic Nerve fibres) |
| 2. |
Absence of corneal reflexes |
V |
VII |
| 3. |
Absence of cranial nerve response to pain |
V |
VII (and limb motor responses) |
| 4. |
Absence of Vestibulo-ocular |
VIII |
III, VI |
| 5. |
Absence of gag and cough reflexes |
X |
IX |
| |
|
|
|
Table II. Clinical Testing For Absence Of Brainstem Reflexes
- The PaCo2 should be 5.33 kPa (.40mmHg) prior to testing and should rise to at least 6.66kPa (50mmHg) during the test.
- The patient should be pre-oxygenated with 100% oxygen for 10 minutesprior to testing & baseline arterial blood gases should be taken.
- Disconnect patient from ventilator but oxygen should be administered at 6 litres/min via a fine bore catheter down the endo-tracheal tube
- Observe patient for 5 to10 minutes for any respiratory effort andensure PaCo2 has risen above 6.66kPa (50mmHg) by repeating arterialblood gases.
- Reconnect patient to the ventilator.
- Discontinue testing if any hypotension, cardiac arrhythmia's or hypoxia occurs
|
Table III. Aponea Test For Confirming 'Brainstem Death' 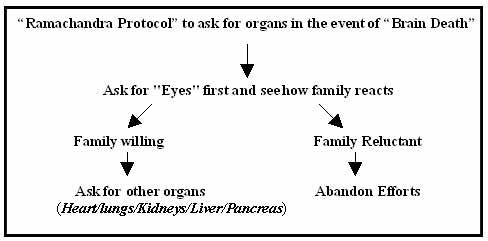 Table IV. 'Ramachandra Protocol' To Ask For Organs
Table IV. 'Ramachandra Protocol' To Ask For Organs 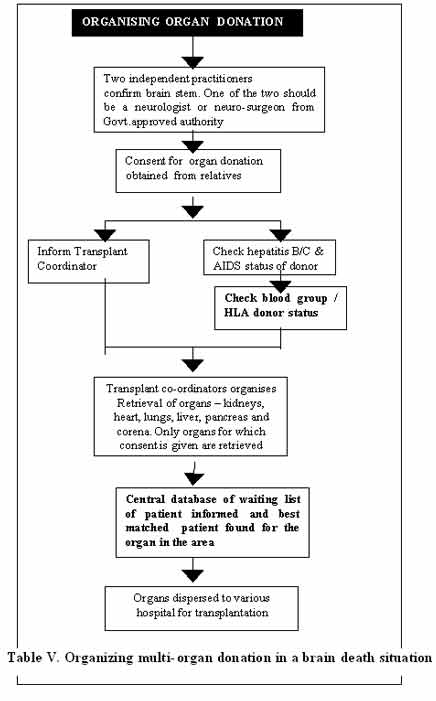 Table V. Organizing multi-organ donation in abrain death
Table V. Organizing multi-organ donation in abrain death
| Corneas |
0 100 years |
(poor eyesight not a contraindication) |
| Heart Valves |
0 60 years |
(Heart Attack not a contraindication) |
| Trachea |
15 60 years |
|
| Skin |
16 85 years |
|
| Kidneys |
0 75 years |
(Paediatric donors are assessed according to weight and size) |
| Liver |
0 70 years |
(size matching is usually recommended) |
| Heart |
0 60 years |
(if unsuitable heart valves may be donated) |
| Lungs |
0 60 years |
(individual assessment of each lung performed |
Table VI. Different Age criteria for organ donation
- Testing for HIV, Hep B & C on all donors.
- Additional tests for syphilis, cytomegalovirus and toxoplasmosis may be necessary
- Virology testing is performed after the completion of brain stem death tests but before the ventilator is discontinued.
- Virology screening is done after consent from next to kin.
|
Table VII - Virology Screen For Brain Dead Patient When Organ Donation is Being Considered
Common Clinical Problems Of Brain Stem Dead Patient
- Hypotension
- Hypothermia
- Endocrine Disturbances
- Electrolyte Imbalance
- Arrhythmias
- Hypoxia
Uncommon Clinical Problems
- Coagulopathy
- Neurogenic Pulmonary Oedema
|
Table VIII. Common & Uncommon Clinical Problems in Brain dead patients
| CARDIOPULMONARY |
|
| Systolic blood pressure |
100-120mmHg |
| Mean arterial pressure |
>60mmHg |
| Central venous pressure |
8-10 mmHg |
| Hemoglobin |
10gm/dl |
| Hematocrit |
30? |
| (Arterial blood gas)pH |
7.37-7.45 |
| Pa |
O2 >75mmHg |
| PaCO |
2 40mmHg |
| SpO |
2 95? |
| RENAL |
|
| Urine output |
1-2ml/kg/hr |
| Core temperature (rectal) |
>35 *C |
| METABOLIC |
|
| Correct glucose and electrolyte abnormalities |
Na+, K+, Ca++, PO4-, Mg++ |
Table IX. Management goals supporting the brain stem organ donor Table I.Form 8 of THO Act
Table II.Cranial nerve reflexes
Table III. Apnoea Test
Test- IV. Ramachandras Protocol
Test-V. Transparent Co-ordination
Test-VI. Age for organ donation
Table VII - Virology Screen For Brain Dead Patient When Organ Donation is Being Considered
Table VIII. Common & Uncommon Clinical Problems in Brain dead patients
Table IX. Management goals supporting the brain stem organ donor
Fig.1. Cause of Brain Death
Fig .2. Testing for Brain Death